Retake
N22) Sore throat, fever, and lymphadenopathy in a college student
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with sore throat and fever.
- Review the DDx considerations in a patient with sore throat and fever.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with sore throat and fever.
History
An 18-year-old college freshman presents to the urgent care clinic with a three-day history of severe sore throat, high-grade fever, headache, fatigue, difficulty swallowing, and palpable swollen lymph nodes in the neck. She reports sharing drinks while consuming alcohol at a party last weekend. Currently, she resides in a dormitory and recently entered a new relationship.
Physical Exam
Vitals: Blood Pressure (BP): 117/73 mmHg, Heart Rate (HR): 92 beats per minute, Respiratory Rate (RR): 24 breaths per minute, Temperature (Temp): 38.5 C (101.3 F), Oxygen saturation (O2 sat): 98% on room air.
HEENT: Tonsils are bilaterally enlarged and erythematous. Both anterior and posterior cervical lymph nodes are palpable and tender to palpation.
Abdomen: The spleen tip is palpable 2 cm below the left costal margin.
Labs
White Blood Cells (WBC): 11,000/microliter (reference range: 4,500-11,000/microliter);
Lymphocytes constituting 51% (reference range for lymphocyte percentage: 20-40%). Atypical lymphocytes noted on blood smear.
Monospot Test: Positive
Provisional Diagnosis
Select the Dx you believe is most appropriate
Considering the patient's history (symptoms consistent with infectious mononucleosis, recent potential exposure at a party), physical exam findings (fever, erythematous and swollen tonsils, palpable anterior and posterior cervical lymphadenopathy, and possible splenomegaly), and lab results (elevated white blood cell count with lymphocytosis and atypical lymphocytes, and a positive Monospot test), the most appropriate diagnosis is infectious mononucleosis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires routine workup and management.
First Imaging Study
What is the first imaging study you will order?
No imaging is required in this case as the diagnosis is primarily clinical. However, we show the findings of a maxillofacial CT with IV contrast in the event that it had been obtained.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
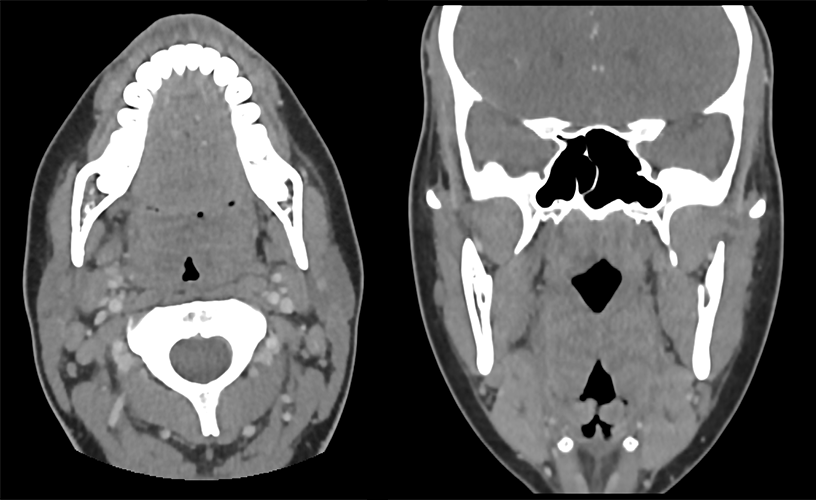
Head and Neck CT
The enlarged tonsils show what type of enhancement pattern?
The tonsils demonstrate a striated enhancement pattern, sometimes referred to as a “tiger-stripe” appearance, which reflects inflamed enhancing mucosa with edematous submucosa
There is an abscess.
There is no evidence of a ring enhancing lesion with a hypodense center to suggest a peritonsillar or tonsillar abscess.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No imaging is required in this case.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
This patient is presenting with viral tonsillitis secondary to infectious mononucleosis, which is caused by Ebstein-Barr Virus (EBV).
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires routine workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is an 18-year-old female presenting with infectious mononucleosis. Her management plan will primarily revolve around symptomatic relief. This includes staying well-hydrated, ensuring adequate rest, and using over-the-counter analgesics and antipyretics as needed for pain and fever control. Given the splenomegaly secondary to the condition, it is important to advise her to refrain from contact sports or strenuous physical activities for at least a month to reduce the risk of splenic rupture.
In light of the incidental finding of a thyroid nodule, a follow-up ultrasound for active surveillance should be scheduled. The nodule currently lacks concerning features that would necessitate a biopsy.
The patient also presents with an atelectatic sinus, also known as “silent sinus syndrome”, an issue with potential long-term and cosmetic implications. She should be referred to an otolaryngologist for further management.
Lessons Learned:
- Tonsillitis, presenting with symptoms such as a sore throat and difficulty swallowing, can be secondary to bacterial or viral organisms. Infectious mononucleosis is a viral cause typically transmitted through body fluids (e.g., sharing drinks), sexual contact, blood transfusions, and organ transplants.
- It's important to distinguish between tonsillitis secondary to infectious mononucleosis and bacterial tonsillitis, as their management differs. A detailed history, thorough physical examination, and appropriate laboratory tests are essential for accurate diagnosis.
- Diagnostic imaging is generally not necessary for infectious mononucleosis unless complications are suspected. However, for severe tonsillar swelling or suspicion of complications, such as an abscess, a maxillofacial CT with IV contrast may be ordered.
Socioeconomic Factors: Infectious mononucleosis is commonly known as the “kissing disease”. Young patients should be informed of the importance of not sharing drinks and STD discussion with partners.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}